Lots of people have had their appendix removed. Others have had their gallbladder, tonsils, or wisdom teeth surgically removed due to issues that arise from their continued presence. Most often, people function normally without these structures present. The shoulder also has a structure that can become problematic, but doesn’t add much to the function of the arm. That structure is called the proximal biceps tendon. Let’s learn more.
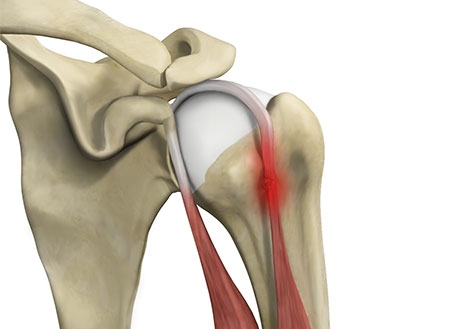
The biceps brachii is the main biceps muscle that allows you to bend your elbow and turn your palm upward. It has two proximal attachment sites: the long head runs through the bicipital groove and attaches to the glenohumeral (or shoulder) joint itself and the short head attaches to the coracoid process of the scapula. This anatomy differs from the muscle’s since attachment at the elbow, which can be more detrimental if ruptured. The long head of the biceps tendon is often problematic for patients. It can become irritated and inflamed such as in the presence of tendonitis. This irritation can lead to partial tearing that results in swelling and leaves the tissue more susceptible to rupture with any kind of trauma-most commonly heavy lifting or pulling.
When this tendon ruptures, patients often report hearing or feeling a pop and experiencing instant pain. Oftentimes, patients then notice bruising or swelling. They typically notice that their biceps muscle now resembles that of Popeye with a noticeable bulge right in the middle. It may sound contradictory, but once these acute symptoms have resolved, patients often feel improved compared to how they felt leading up to the injury.
Because the biceps muscle has a secondary attachment site, the arm is still able to function without the long head intact. Therefore, it is rare that an orthopedic surgeon will recommend repairing this biceps tendon. In fact, for patients who struggle with chronic proximal biceps tendon irritation, our surgeons will actually surgically release the tendon. They can either cut it and re-attach it to the superior aspect of the bicipital groove (tenodesis), or they can simply cut it and leave it be (tenotomy). The only difference in these procedures is the cosmetic deformity (Popeye) that results from the tenotomy. These procedures are not typically performed independently. Rather, an MRI would be obtained and your surgeon would likely perform a debridement (or clean out) procedure in your shoulder as well. The recovery from this type of surgery is minimal compared to a rotator cuff repair. If a tenodesis is performed, the tendon does need some protection to allow it to heal. Otherwise, activity as tolerated is often the recommendation.
Regardless of whether you have a healthy tendon, a ruptured tendon, or a surgically released tendon, your arm is likely to function similarly. Whatever your circumstances may be, let our board-certified physicians guide you through the process!